
Ganglion Cyst
Ganglion cysts are masses usually found around the wrist, although they can be found in other places.
The term "ganglion cyst" actually is a very poor term for a wrist mass, since the two terms can refer to many other things. That is, the term "ganglion" is unfortunate since that term also refers to a grouping of nerves, and "cyst" is an unfortunate term since it can refer to any number of kinds of fluid collections: breast cysts, brain cysts, bone cysts, etc.
The ganglion cyst is not associated with nerves, but with joints and tendon sheaths. Ganglion cysts are small outpouchings of joint capsule (the sleeve of tissue that encloses a joint) if they are found around a joint,, or tendon lining tissue if they are found near a tendon. In general, ganglion cysts consist of an outer fibrous coat and an inner lining, and contain a clear, colorless, gelatinous fluid.
Dorsal Wrist Ganglions

Dorsal Wrist Ganglion. Photograph courtesy of Dr. Burns
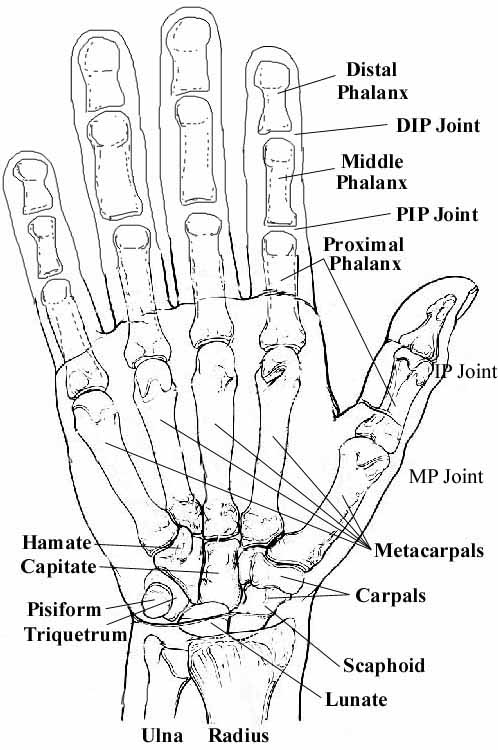
The most common ganglions of the hand are dorsal (back side) wrist ganglions, which are outpouchings of the wrist joint capsule. They arise from the scapholunate ligament (you can see an illustration of this ligament on the Arthroscopy page, colored green, on the lower left side). Volar (front, or palm, side) wrist ganglions come from the scaphoid-trapezial-trapezoid (STT) joint. (You can see the bones of the wrist here. The trapezium and trapezoid are not labelled; they are the two small bones next to the scaphoid). The picture at the top of the page is a typical dorsal wrist ganglion, occurring at the wrist joint. They can also be on the palm side of the wrist, as seen below in an example of a volar wrist ganglion.
 |
 |
|
The volar wrist ganglion is near but not at the wrist crease |
Here is the ganglion at surgery. It is a lumpy, tan sac filled with joint fluid held by the forceps on the right. |
Other Kinds of Ganglions

{kind=link}
There are two other types of ganglion cysts that are common in the hand. A ganglion cyst associated with arthritis of the DIP joint (the one closest to the fingertip) is called a mucous cyst (see photograph below). A ganglion cyst associated with a tendon is called a tendon sheath ganglion or a retinacular cyst, and is usually a small, very hard, 2-4 mm ball at the base of the finger, on the palm side. These latter two types have a number of special characteristics that are not covered on this page. I will discuss these with you during your visit.
All ganglion cysts ("cyst" just means fluid-filled container or hole) are, as I stated above, outpouchings of joint capsule, which is the sleeve of tissue that encloses a joint, keeping in the lubricating joint fluid. The tendon sheath ganglion arises from the similar lining of a tendon, but only when that tendon is one that is enclosed in a structure analagous to a joint capsule. The reason for this is that most joints and some tendons have their contents under pressure or stress because of the way the system is loaded. In all probability (although this has not been proven) the ganglion represents a form of "blow out" of this enveloping sleeve around the fluid filled joint or tendon sheath. Once formed the ganglion may then grow by either continued leak of fluid under pressure or (some suggest) by the formation of a one way valve effect betweemn tha joint and the cyst. What is certain is that the joint becomes filled with a jelly that is clear and viscous and contains some of the constituents of the joint fluid (itself a very specialised fluid adapted to lubricate and nourish the joint structures).
When to Treat a Ganglion
Ganglions become symptomatic when they grow large enough to be obtrusive, or when they compress surrounding structures causing pain, or rarely they can cause nerve damage from compression. They are very common and also very poorly understood. We are not entirely clear on the causes of gangions or even what will happen if they are not treated. They are common in young or middle aged people but rare in the elderly. Do they just go away by themselves? Some good evidence exists to suggest that they do spontaneously grow smaller or go away in time, but this may take years or even decades. Some ganglions will continuously enlarge, especially if they are due to arthritis.
How do You Treat Ganglions?
One form of simple treatment is aspiration of the contents, but this is usually only a temporary solution. The ganglion may become less tense and less painful but they almost always come back, sometimes within days or weeks. Injection with steroids usually does not improve the results of aspration alone.
Excision (surgically removing it) is indicated if the ganglion is causing local pressure effects or pain (common on the back of the wrist), or is so big it is unsightly. Recurrence does happen (about 10%), and is usually related underlying pathology. Mucous cyst ganglions are a problem due to the prominence at the finger joint, and may recurrently drain. Tendon sheath ganglions usually hurt when you grip, because they are found just under the skin but overlying the bone.
If you would like to read what some patients have written about their experience having their cysts removed surgically, click here.
Ganglions are the most common mass around the wrists, so there is a lot written about them. You can select from:
American Society for Surgery of the Hand: CTS Patient Education Brochure.
Dr. Charles Eaton, an excellent Orthopedic Hand Surgeon in Florida, and a friend: Ganglions. Once you go to this page, select "Alphabetical List" and then "ganglions."
| Would you like to search the medical library of the National Library of Medicine for scientific papers on this topic? Just click on the Pub - Med image: | |
| Remember the admonition from the Patient Education Links Page: the Internet has a lot of information, much of it incorrect. I have reviewed the sites that I have linked to, and have only linked to sites when I personally know the surgeon who posted it, or am a member of the organization that posted it. However, I may not agree with all that is on that site, and it may have changed since I reviewed it. If any of the information is not consistent with what I have told you, please download the material and bring it in. | |