
Locked MCP Joint
CASE HISTORY
67 Year old woman jerked a gallon of milk out of a display case in the grocery store. Her third finger through fifth fingers were in the handle, the third finger was jerked ulnarward and she thereafter could not extend the third MP joint. Came to ER, where Xrays were normal and showed no fx or dc. The ER MD could not think of any explanation other than a dislocation, so she blocked the finger and could not "reduce" the located joint (could not extend the MCP, either). The ER MD called the MD on call for hand, who came in to see the patient. She could not think of any explanation other than a dislocation, so she blocked the finger and could not "reduce" the located joint (could not extend the MCP, either). So hand surgeon called me for suggestions. I considered that the patient might have the MC head buttonholed through the extensor hood or a split extensor mechanism with part of the hood or one of the interossei stuck below the MC head. The hand surgeon asked me to hold and re-examined the patient: the extensor mechanism seems midline and normal. I suggested that she go to the OR, open it up, and see what was preventing extension. The patient decided to see me.
On physical examination, the extensor mechanism looked perfectly normal and was centralized with no subluxation, and no puckering of the skin. The, DIP and PIP joints worked normally, just no MCP extension. Xrays showed a good-sized osteophyte on the 3rd MC head but no dislocation. I was not sure of the diagnosis but suspected the collateral ligament might be caught on the osteophyte.

Three views of the hand; note the foreshortening on the PA and Oblique
due to the inability to extend the MCP joint: note the flexed MCP
on
the lateral view
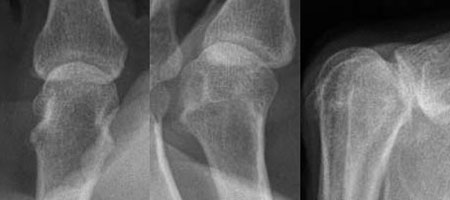
Detail views of the third MC, with osteophyte on ulnar (left) side of joint
I ordered an MRI, which was read by David Stoller, MD, the author of the textbook on MRI of the musculoskeletal system. I discussed the images with him on the phone: a bit of fluid around the MCP joint with some interossei swelling, but nothing abnormal detectable on the extensor or flexor mechanisms. He could not see anything caught on an osteophyte, but felt the detail of the study might not be good enough to detect that.

Two images from the MRI
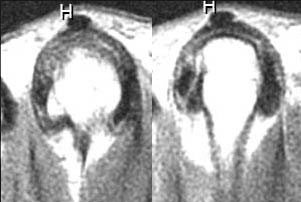
Details of the above showing asymmetry of the
joint with the osteophyte (left image) and a fluid
layer on the same side as the osteophyte within
the substance of the collateral ligament (right image)
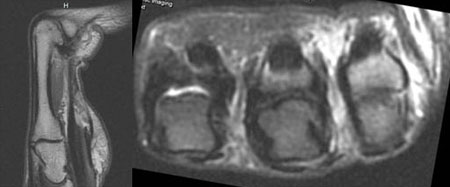
Additional MRI views
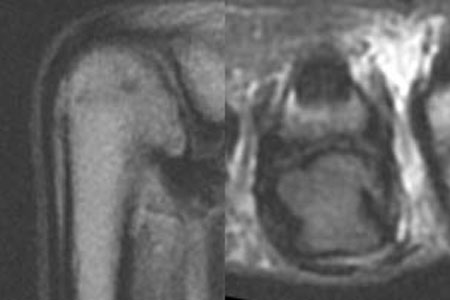
Details of the above MRIs.
I decided to explore the joint from the dorsal side.
Surgery Findings
Culprit: Accessory collateral ligament caught on a large volar osteophyte. The incision:

The dissection was deep given the small incision. I could see the collateral ligament, which appeared to be caught, but the limited exposure made this difficult to determine definitively.
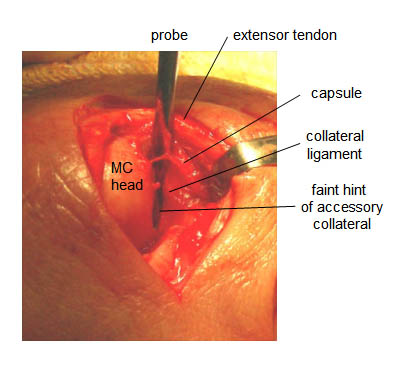
I could not free up the collateral ligament, even with a probe. I finally decided to cut the accessory ligament part that was caught. Finger moved normally immediately afterward. I then took a small curette, reached down the hole, and somewhat blindly removed as much of the osteophyte that I could. In the view above, the "faint hint" of the accessory collateral can be seen crossing the probe, in this photo from left top to right bottom. It was clearly visible at surgery with loupes. This is the band that I cut that allowed full extension.
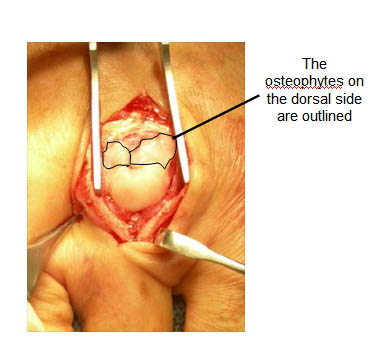
There was a large, about 4mm x 6 mm area of MC head with a full-thickness defect just slightly volar to this view, causing the formation of large osteophytes. I could not photograph the volar ostephytes, as the incision was too small and the osteophyte was deep. The large dorsal osteophytes, which I removed, are shown.
I did not repair the collateral ligament, it was lying exactly where it should, since it was not completely released. I repaired the EDC with simple 4-0 Ethibond buried sutures. Even without repair, the extensor mechanism worked great without gapping, so there is minimal stress on the repair.
| Would you like to search the medical library of the National Library of Medicine for scientific papers on this topic? Just click on the Pub - Med image: | |
| Remember the admonition from the Patient Education Links Page: the Internet has a lot of information, much of it incorrect. I have reviewed the sites that I have linked to, and have only linked to sites when I personally know the surgeon who posted it, or am a member of the organization that posted it. However, I may not agree with all that is on that site, and it may have changed since I reviewed it. If any of the information is not consistent with what I have told you, please download the material and bring it in. | |